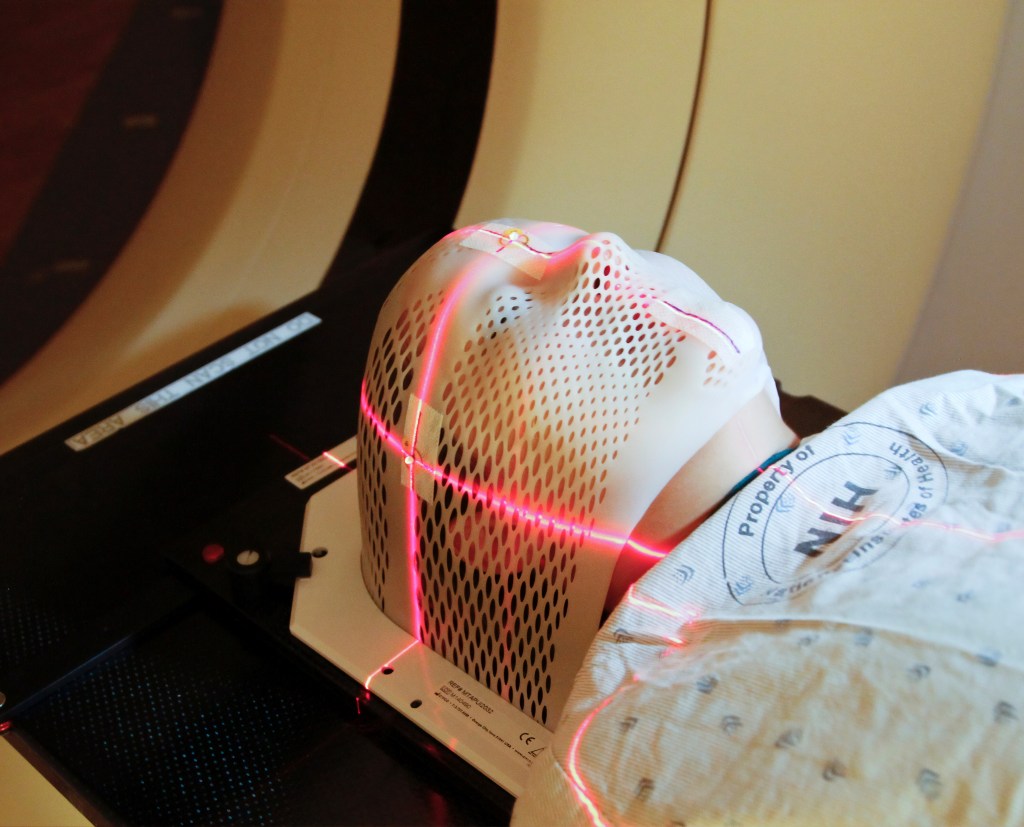
Many of us who have lived through early stage breast cancer with lumpectomy surgery have also gone through radiation treatment.
If you’ve been there, you know the drill: 4-6 weeks of daily radiation sessions. Each one is relatively short, but there’s the time involved in getting there, changing into a gown, waiting for your turn, having the treatment, changing back into your clothes and getting back home (or work or wherever else you need to be).
And this happens every single day, five days a week, for weeks. You get to know your radiation therapists very well. And they get to see your breast over and over again. It goes on and on and on.
Closing the book on cancer treatment is a great feeling. And making radiation even shorter? Yes, please!
Women who have an elevated risk of having the cancer recur at the tumor site are usually given an additional “boost” of radiation to that area. This takes place after the initial weeks of radiation, extending the length of treatment. However, researchers discovered that this boost could be given concurrently, thereby shortening the number of weeks that patients had to undergo radiation without compromising its effectiveness.
From the perspective of a patient, this is very welcome news. Setting aside time every day of the week to make the trip to the cancer center for treatment only works if your other responsibilities are flexible. I was working part-time during this, had access to a car, could get to the cancer center quickly and could be done in time to pick up my kids without too much of a problem. My bosses were extremely understanding and gave me the latitude I needed to complete my treatment with a minimum of stress.
For many, however, this might not be the case. Being able to shorten the overall treatment time could be critical in helping patients finish all their sessions.
It is heartening to know that as cancer treatments evolve, they become much easier to incorporate into our everyday lives. I am hopeful that the changes that come about over the next 10 years will provide even more options for successful completion of treatment with a greater survival rate for all.
Note: the results of the referenced clinical trial were presented on Oct 24, 2022 at the American Society for Radiation Oncology (ASTRO) annual meeting in San Antonio, Texas with Frank Vicini, MD as the study leader. My expectation is that more information will be published and I will try to post it here once it is.
From what I can tell, the loss of body odor following cancer chemotherapy isn’t widely acknowledged within the medical community, but it’s certainly something that many of us have experienced.
This is NOT what you think of when someone says, “sweaty armpit”!
Based on what I’ve read, this might be a result of the weedwhacking effect that chemo drugs have on our microbiomes. Regardless, the result has been positive for those of us who find that we don’t have to worry about being smelly.
However, I happened to catch an interview on National Public Radio (aka NPR) that helped make more sense of what was actually going on, even though it was a bit of a killjoy. Listen to it here, where you can also find a full write-up of the piece.
Basically, that sweaty stink that we find repugnant is from a compound produced by bacteria living on the skin. One species of these bacteria that’s associated with an onion-like odor is Staphylococcus hominis.
Our stinky sweat may offer some protection from stuff like MRSA, shown on this CDC photo. They might look like cute fuzzy purple balls, but in the age of antibiotic-resistant bacteria, they’re potential killers.
And unfortunately, these smelly microbes are very beneficial, helping protect humans from things like eczema and MRSA (antibiotic-resistant Staphylococcus aureus). As one of the researchers puts it, sweat is an “antibiotic juice” that forms a protective layer on our skin as it dries.
Yeah, I know what you’re thinking: cancer is miserable enough, and you HAD to take away this one little thing (loss of body odor) that was the only perk to chemo?
Well, as mentioned above, I’m not qualified to definitively say that it’s the chemo that kills the skin microbes and makes you not smell. I’ve been unable to find research studies that examine the effects of chemotherapy on your skin’s microscopic residents. Nonetheless, I’ve tried to contact the researchers mentioned in the NPR story to see if they’ve had any experience with chemotherapy and loss of body odor in cancer patients. If they reply, I’ll report back to you.
For now, if you’re happy being odorless, keep enjoying it.
I’ve shared that I recently completed a three-month, 200 hour Yoga Teacher Training (YTT).
My main motivation for entering YTT revolved around yoga’s role in my emotional recovery from cancer. My teaching goal is to make yoga accessible to more cancer patients and survivors. Sadly, the view that many have of yoga in the USA is that it’s mainly for young, white, flexible, affluent women.
That means that the benefits of yoga are not reaching many of the populations that need it most.
Sadly, yoga in the USA is not associated with a diverse clientele.
In YTT, I expected to deepen my own practice, immerse myself in the roots of yoga and gain experience in sequencing and teaching among other things. And we did that. The program was well-rounded and paid homage to yogic philosophy, in addition to covering a broad range of relevant topics such as anatomy, meditation, sound healing and creating an inclusive atmosphere.
What I didn’t expect was what I learned about myself. Now, in the course of cancer treatment I gained access to counseling at my cancer center with an excellent therapist. And prior to that, I had sought help for anxiety. I’d explored talk therapy, cognitive behavioral therapy (CBT), eye movement desensitization and reprocessing (EMDR), mindfulness-based stress reduction (MBSR) and had gone through a lot of introspection. Basically, I thought I’d covered my bases and knew what’s what when it came to my inner workings.
YTT proved me wrong. I learned that I still struggle with competitiveness, perfectionism and a host of little insecurities. Wow, that was an eye-opener, even after all the “head work” that I’d done! In addition to coursework, YTT had a requirement of attending a number of yoga classes. Due to the limitations on my time given my work and family schedule, I was forced to take the heated (~95F) Level 2 classes, which happened to be most convenient. They emphasized balance and flexibility, while my non-yoga fitness focus has been strength and endurance.
*ahem* This is NOT me.
Balance and flexibility against the backdrop of neuropathy, menopause and vestiges of cancer treatment effects did not allow me to show my “best side.”
Not a big deal, I thought, since yoga for me is a mental “work-in”, not a workout. I’ve felt that holds truer to the traditional purpose of yoga and respects its roots. But in a crowded yoga studio where I was usually the oldest class member, I struggled to maintain my composure. Many of the other students could have been my offspring. The Level 2 classes made me look, I felt, like I didn’t belong.
And that feeling got worse as the classes went on. By the last weekend, I was the only teacher trainee who showed up (others trainees had more flexible schedules that allowed them to take other classes). After weeks of taking Level 2 classes, feelings of dejection had built up.
I should be over this, right? I should have been able to hold my head high and do what I could, knowing that my fitness stemmed from other activities and yoga served a different purpose for me than for “the youngsters”.
But nope.
The YTT itself was exceptional and the teacher trainers were amazingly supportive and knowledgable. The other members of my class were (no surprise) all white, all female and all younger than me. But they were generous and sweet and each one had been through her share of hardships. I felt only love from them. I just didn’t feel it from myself.
This is my preference for yoga: slow , mindful movements performed with intention. No contortions.
And with fitness being so important to me, I was frustrated that yet again I managed to find a situation where I showed myself to be “less than”. That was painful.
Yet, this peek into my current state was invaluable. Being in the midst of all those younger bodies strengthened my resolve to create classes that are more suitable for not only cancer folk, but also for other special and older populations.
YTT taught me that I don’t have it all figured out yet. However, it also gifted the awareness of what was really going on. Just as in mindfulness meditation, once I became aware of where my mind was leading me, I could take action to return to a place of peace and acceptance. That advanced my emotional evolution by lightyears!
Experiencing classes at a yoga studio also drove home the necessity of offering yoga to people who would benefit from the practice but are often forgotten when classes are planned. There are populations for whom studios are simply inaccessible financially, physically and even psychologically.
Ultimately, this next-level awareness showed me that what I had been doing on my own over the years still counted as yoga, even when I didn’t look like the other class members. It was the yoga I needed. And that was enough.
[IMPORTANT: Please be aware that at the time the videos were filmed, I was in a very negative headspace. My experience should not be considered an example of a “typical” experience because with cancer treatment, there is no such thing. Just as cancer is a disease specific to an individual, so is the treatment and, as a result, one’s response to it. If you are interested in viewing the below videos, please keep all the above in mind.]
I’ve posted quite of few photos of my cancer journey. You’d think I wouldn’t have any more pics left, but–surprise–I do!
I made some important (to me) videos after my sixth and final infusion, but to date I’ve hesitated to post them. In part, this is because I’ve tried to remain anonymous in this blog, but in the clips, you get to see my face. And it’s not a pretty sight.
I didn’t feel human.
I was the weakest that I’d been my entire adult life. My body was feeling the strain of multiple infusions of chemotherapy, I didn’t recognize myself in the mirror and my voice didn’t sound like my own. I was so sick and tired of this part of the treatment and wanted it to be DONE.
At this point, I wasn’t suffering that entire cascade of side effects that I’d experienced after my first chemo infusion, and I’d learned to better deal with what I did experience, and even what to do to avoid some of the side effects.
However, the fatigue I felt was far beyond what I imagined it would be. And it was coupled with constant background nausea, like a slow burn in my gut. This was a result of losing the rapidly-dividing cells that lined my intestinal tract; they were felled by the chemotherapy, collateral damage as the medicine killed off potential cancer cells.
Strangely, there were also times when I was actually quite hungry, but literally too tired to try to get something to eat. Even calling for a member of my family to bring me food required too much effort. Speaking took a lot of energy.
The final infusion’s side effects lasted the longest. A full week after my infusion I was still very unsteady and barely made it to work for a few hours.
It’s worth noting that this was pre-pandemic and I wasn’t properly set up for working from home. Were I experiencing chemo treatment now, I’d be able to get more work done…likely to my detriment, unfortunately, because I really needed that time away.
It took five years for me to decide that it was time to post these videos. Apologies if they get a little intense:
Last year at this time, I feared that I had heart issues based on what I had read about some of the cancer medications that I had been on, so I went to the cardiologist and they administered some tests. When I came back to the cardiologist to discuss results with the doctor, I was told that they had found “something” in the echocardiogram and Holter monitor readings.
But I still had questions, so I had a consultation with the cardiac nurse, who went through everything with me.
In the back of my mind, there’s a fear that my body is harboring serious health problems.
And it turns out that while they did find “something”, it wasn’t really anything out of the ordinary, beyond normal wear and tear. I was assured that my heart was very strong and healthy and I could continue to push through high-intensity workouts.
Still, it was recommended that I get checked out again this year.
But you know what? I’m not going right now. It felt like anxiety about the scans and then waiting for the results did worse things to my heart than whatever I might have been already experiencing.
I talked this over with my oncologist, who agreed.
The fact is, there are things that you need to get checked out, especially as a cancer survivor. But for other things, especially without a specific indication that there’s something wrong, you are simply looking for trouble. And if you’re looking for it, you’re going to find it.
Our bodies are not perfect. And the older we get, the more aches, pains and abnormalities we have. That doesn’t necessarily mean that there’s anything “wrong” that immediately needs to be fixed.
For now, I’m halting my search for trouble and taking the time to breathe deeply and just live.
Anxiety was the driver for me to get tests run. I was overreading about everything that could possibly go wrong–given the medications that I had been taking–and then rushing out to make sure that it hadn’t yet in the hope that I could rectify any budding issues.
And to be fair, there are still things that I could look at, still specialists I could contact. But perhaps I need to chill a bit…
…but perhaps I need to chill a bit. If it were to progress, would I stop exercising? Absolutely not. So then perhaps it’s best to take a wait-and-see approach for now.
All of this is so different from cancer, which drives us to seek treatment immediately. I am forever primed to worry about what might be happening in my body. But I also recognize this as a psychological side effect of cancer. I can’t let fear take over the rest of my life.
So for me, it’s time to stop looking for trouble, stop fearing for the future and simply relax and enjoy what’s happening in the present moment.
After finishing chemo for breast cancer and noticing that I had no body odor, I decided to write a post about it because the Internet was silent on the topic. Apparently, I wasn’t the only one who’d come up empty. A number of you commented that you’d noticed the same thing and similarly found no explanation.
Well, five years after my initial diagnosis, maybe 4.5 years after finishing chemo, I still can’t locate info on the Internet about this.
If I do find the odd article about cancer and body odor, it’s about the exact opposite: smelling bad as a result of the disease or certain medications. Not what I’m looking for.
Hey, Internet! Is there really no one looking into this?
It is quite weird that I can’t even find anything in the US National Institutes of Health PubMed database, so I would suspect that chemo-related loss of body odor is not on the radar of researchers. Well, it’s certainly not on my oncologist’s radar because he said he’d never heard of it and didn’t think it could be attributed to chemotherapy. Personally, I can’t imagine how it could be from anything else.
I’m going to pester him about it again during my next appointment. Usually armput odors are caused by bacteria. As an article from the Cleveland Clinic explains, odor is produced “when bacteria on the skin break down acids contained in the sweat produced by apocrine glands, which are located in the armpits, breasts, and genital-anal area. The bacteria’s waste products are what produce the smell.”
And NPR ran a story on researchers looking into what the worst bacterial offenders are, noting, “When the bacteria break down the sweat they form products called thioalcohols, which have scents comparable to sulfur, onions or meat.” The greatest culprit? Staphylococcus hominis.
So then maybe the chemo stops the production of thioalcohols? Or chemo wipes out the S. hominis living on our skin? I’m surprised that no one is researching this in the context of chemo patients, because it seems like it might have some health implications. We still don’t know all the side effects of chemo drugs and it would be useful to start a conversation about this one.
If you’re experiencing this, please tell your medical team. They might simply not be aware of what’s happening.
I’m not saying that I smell like a bouquet of flowers, but according to my husband, there’s no “sweaty pit” odor.
And you might be wondering what my current experience is, almost five years later. Even though I departed the realm of the completely-odorless about two years after completing chemo, I still have very little body odor. And it’s not like I don’t give it chances to fester since I work up a good sweat when I exercise. Note that my left armpit, which was thoroughly irradiated, exudes almost no noticible odor. My right armpit doesn’t smell very much, but sweat that gets on, say, a sports bra will start making the fabric stink the next day. (Let’s just say that I’ve been testing this out.) The skin in the armpit itself? Minimally, and that’s with no deodorant, although I do wear it anyway.
Certainly, the six weeks of radiation therapy on my left side would likely have an effect, and so it would make sense that there’s a difference in odor between both armpits.
Still, the “natural” (and unfortunately overpriced – yeesh!) deodorants do a very good job of fragrancing my armpits because they don’t have to work very hard.
So the mystery remains. I’m going to keep digging into this as it’s likely there’s a disruption of our skin microbiome involved, and given the popularity of that research (see microbiome and armpit odor info at drarmpit.com), someone may be looking into the connection between chemo and body odor in the future. Until then, I’ll just remain happy and relatively unstinky with fingers crossed that it continues.
~~~~~~~~~~~~~~~~~~~~~
Many thanks to my very patient husband who played along and agreed to smell every place I pointed to. I’ll revisit the odor issue during the summer just in case…
Running late with this post as I’m furiously cleaning our apartment in advance of the Christmas holiday!
I noticed a few mornings ago that when I made a fist and then straightened the fingers of my right hand, the joints didn’t stick at all.
It took over 300 days…but I’m happy to celebrate the end of the side effects!
While this may seem like an odd thing to celebrate, it marked a milestone for me. This was the last side effect attributable to letrozole that I had been experiencing, and it was finally gone. Letrozole is an aromatase inhibitor that blocks production of estrogen and is used as endocrine therapy for breast cancer patients who have estrogen receptor-positive tumors. I’d been on it for about 14 months after switching to it from tamoxifen.
For reference, as of today, I am at Day 307 since stopping the medication, so it’s taken quite a while for this joint side effect to subside. Yes, there are other things still plaguing me, such as memory issues, low libido and difficulty maintaining muscle (even with strength training), but those are more difficult to separate out from the garden-variety effects of menopause.
The sticking fingers began in August 2020 (about 8 months after starting letrozole) and were getting progressively worse. By March 2021, when I called it quits with the endocrine therapy, a number of finger joints were sticking and painful, particularly in the morning.
At that point, I was having trouble getting up off the floor, as I was having issues with joints throughout my entire body. The medication was affecting various aspects of my life, making it difficult to exercise and, as I like to put it, lowering the quality of my existence. Following discussions with my oncologist, we both agreed that my risk of breast cancer recurrence was low enough to stop the meds.
It’s been quite a journey to get to the point where I am now.
Shaking this last side effect of letrozole reminded me how far on this cancer journey I’ve traveled. There have been so many ups and downs, friends made and friends lost to the disease, that it was easy to forget that nothing in life is permanent. Time passes and situations change, sometimes for better, sometimes for worse.
The concept of “CANCER” used to terrify me, and after I was diagnosed, I hit a low so deep I thought I’d never be able to crawl out of it.
Gradually, as my experience with the disease played itself out, I came to accept the uncertainty about the future. As the end of 2021 draws near, I inch closer to the 5-year survival mark. The fact that I can straighten my fingers in the morning without any pain or sticking is a perfect example of how while I cannot know what the future will bring, I can deal with the “now”. And this “now” is not so bad.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
Best wishes to everyone for a very Joyous Holiday Season and much promise for 2022!
The last time I was researching the link between cancer and sleep, noting the myriad benefits gained from solid nighttime rest, I was surprised to see mention of melatonin’s role in decreasing the risk of cancer.
For anyone who might not be familiar with it, melatonin (a tryptophan derivative) is a naturally-occuring hormone secreted by the pineal gland that signals when it’s time to sleep and wake. It’s mediated by light levels, with the amount of melatonin in your body increasing as the sun goes down. You’ve probably seen melatonin on the vitamin shelves at your local store, as in recent years it’s been popularized as a non-addictive sleep aid. What I hadn’t realized was that its effect on cancer cells has become an active area of study.
I dug into the PubMed database to find there was quite a bit on this topic. However, note that not all the journals in which these results were published were familiar to me, so I cannot vouch for the rigor of the peer review, however, there was a general consensus that melatonin showed promise.
Melatonin shows a lot of promise as a cancer fighting hormone.
It’s well-established that women who work night shifts experience disruption of their circadian cycle and have an increased risk of breast cancer risk, purported to result from extra circulating estrogen (Cohen et al., 1978, Lancet). Researchers are now linking that disruption with a decrease in melatonin production.
Amin et al. (2019, J Cell Biochem) describe the action of melatonin as it relates to cancer: “Melatonin via its receptors and various second messenger pathways decrease[s] cell duplication and increase[s] cell differentiation.” Since cancer tumors are composed of a proliferation of poorly differentiated cells, this means that the action of melatonin works against the process by which cancer develops and progresses.
Amin et al. continue by noting that melatonin “regulates estrogen-dependent pathways (by nonreceptor-dependent means) and reduces the production of oxidants; as a result, melatonin inhibits cell toxicity and mutations….Melatonin interrupts estrogen-dependent cell signaling and also causes reduced estrogen-stimulated cells in breast cancer. [It] is a mammary tumor inhibitor…[as relates to the] development, progression, and metastasis of breast cancer via a number of molecular mechanisms.”
A randomized, double-blind, placebo-controlled research study showed that melatonin has a neuroprotective effect that can counteract the effects of chemotherapy on “cognitive function, sleep quality and depressive symptoms” (Palmer et al., 2020, PLOS One). These are significant side effects that have a profound impact on the patient’s quality of life, and anything that may relieve these will improve the entire treatment experience.
Griffin & Marignol (2018, Int J Radiat Biol) noted that melatonin administered to subjects before they were exposed to ionizing radiation resulted in the breast cancer cells being more sensitized to the radiation therapy, rendering it more effective. And melatonin seemed to reduce the radiation-induced side effects exhibited by both human and rodent subjects.
No matter how many drug treatments are available for cancer, they do no good if the cancer cells develop a resistance to them. In a study published this year, Sang et al. (2021, Cancer Lett) found that melatonin increased the effectivess of drug lapatinib in HER2 receptor-positive breast cancer cells that were originally resistant to the drug, suggesting that melatonin could be a promising adjuvant therapy for treating advanced HER2+ tumors.
So, melatonin may reduce breast cancer risk, make existing treatments more effective and help protect patients against negative effects of these therapies. Does that mean you should run out and gobble melatonin every night?
Many studies are first run on animal subjects, but to truly determine whether a treatment will be effective for cancer patients, it must be tested on humans.
No! As tempting as it sounds, that’s not an advisable course of action. Many more studies still have to be run to evaluate the exact mechanisms by which melatonin acts on physiological processes. Some of the results in the cited studies were based on small sample sizes; good for proof of concept, but following up with larger scale studies is critical. Some studies were run on animal models which are not the best human analogues. In addition, there’s little direction regarding proper therapeutic dosages. Establishing those will take additional research.
Keep in mind: a naturally-occurring hormone like melatonin likely has a “sweet spot” in terms of dosing, and determining the ideal amount may be tricky. Just because you can buy melatonin gummies in 10mg doses does not mean you should be taking that much.
Furthermore, melatonin may elicit negative side effects in some people, including headaches, nightmares and nausea. Side effects tend to be short-lived with short-term usage but there’s still not enough information available about long-term safety, so taking it for longer periods of time is strongly discouraged.
Note also, the articles I’ve mentioned above were selected because they describe recent research, although some of these are review articles that espouse the authors’ opinion, backed up by research selected for the purpose. If you’d like to read the above studies yourself and the links I’ve posted do not provide you full access, please consult your local university library for copies (copyright laws prohibit me from providing access to pay-only articles, regrettably).
Finally, it may be that some of melatonin’s benefits might be its undoing. Reiter et al. (2017, Int J Mol Sci) note that melatonin is inexpensive and readily available, and therefore there might not be the same level of interest in researching and developing it for cancer use as there might be with a novel drug with the potential to be more lucrative.
Where does this leave us?
I would urge you to: 1) Ask your oncologist about what they would recommend, given the research that’s coming out. They are still your best source for information. FranticShanti.com is only a blog and can be used as food-for-thought but definitely not for determining your course of treatment. 2) Learn how to read scientific studies. There are free courses on educational site such as Coursera.com that explain research design and interpretation in layperson terms. They can offer instruction on reading research with a critical eye. 3) Keep an eye on emerging research. Databases such as PubMed are excellent sources for health research. Even if you’re not well-versed in research design, you can look up articles to bring to your next visit with a health provider. 4) Do not take megadoses of melatonin! There is still so much we have to learn about this hormone as it relates to cancer, and self-medicating with melatonin in the hopes that “maybe it’ll help” is dangerous. Again, your oncologist remains your best source of information.
Promising drugs aside, get your sleep!
I do encourage you to respect your circadian rhythm by establishing good sleep hygiene practices to improve the conditions for your body to create and release its own melatonin. Proper and adequate sleep will always benefit you!
And so we get back to the idea that launched this post: sleep remains the ultimate good.
~~~~~~~~~~~~~~~~~~~~~~~~
It bears repeating: ALWAYS ask your cancer team about starting any new medication or supplement, regardless of how well-supported it is by research.
Ever get the funny feeling that something’s wrong?
Like things are a bit “off” but you can’t be sure? I’ve been dealing with that ever since I got off letrozole, an endocrine therapy for breast cancer with a reputation for being difficult to take.
As of this posting, I’ve been off letrozole for 117 days exactly–yes, I’m counting. I’m still shaking off side effects like stupid-crazy joint stiffness, but at least I can tell things have improved.
That’s not what I’m talking about here.
I’ve taken a few rides in the MRI tube already. Not in any hurry to repeat that.
Right now I’m having some “really intense” memory and focus issues. I’ve put “really intense” in quotes, because I talk in superlatives so that my concerns are taken seriously. It’s a bad habit, especially when speaking to an oncologist, because it’s a sure way to end up in an MRI tube. Again.
In the past, my oncologist suggested that my memory problems might have been related to anxiety and not the medications I was on. That’s quite possible, although it’s hard to tease apart “anxiety” and “med side effects”. I mean, simply being told you have cancer causes an immediate spike of the Stress-O-Meter. For someone as anxiety-prone as me, it’s like I’m constantly red-lining.
Now I’m off the endocrine therapy and my memory and distractibility seem to have gotten even worse. What I had before wasn’t like THIS.
It’s kind of like saying, “This hurts. I think I’m being hit on the head with a hammer.” But then you actually get hit by a hammer, and think, “WHOA, now THIS is being hit on the head with a hammer!”
If thoughts are beads on a string, my beads are dropping off at a constant rate, leaving me wondering what I was about to do three seconds ago. And getting distracted by shiny objects. Couple that with having to learn a complex new financial system for work (grrrrr, Larry Ellison), not having helpful documentation to do so and having to go through that while being mainly confined to my bedroom for over a year…yeah, it’s a mess.
I am not being rational and I know it. But I’m still on high alert and dialing my fears down is going to take time.
Because my breast cancer was HER2+–which has been associated with metastases to the brain–my anxious little self immediately thinks, “Wait, maybe this is cancer’s spread stealing my thoughts???” I think that I will forever be jumping to that as the first possibility.
That’s not completely unreasonable, either. According to “Medical News Today”, memory problems are listed as one of the symptoms of brain metastases, along with headaches, stroke, seizures, confusion, dizziness…okay not really experiencing any of those.
And the Mayo Clinic metastasis website asks: what are the most likely causes of my symptoms? So, I admit, a brain tumor probably isn’t, given all the other more likely possibilities: menopause, work stress, loneliness, lack of purpose…and *cough* listening to Twitch video streams while I’m trying to focus.
So really, these memory issues could be a completely normal effect of menopause, but in the cancer context the possibilities are frightening. It takes a lot of perspective to be able to look at what’s going on and realize that it’s not aberrant or dangerous. I feel like an idiot for jumping to the worst conclusions, but here I am…
Looks like visiting a cardiologist after stopping aromatase inhibitors for breast cancer was a good idea after all.
The letrozole (aromatase inhibitor) that I’d been taking has been associated with cardiovascular effects, and since I was feeling progressively worse from the medication, I wanted to make sure that everything checked out okay.
With the improvement in surivorship comes an increase in the diseases that come about from cancer treatments. The longer people live, the more long-term effects take their toll.
It seems like the American Heart Association (AHA) agrees with my concerns. An April 26, 2021 statement by the AHA underscored the complicated picture of cancer treatments, in this case hormonal therapies for breast and prostate cancer. As stated in the article by Okwuosa et al. (2021) published in Circulation: Genomic and Precision Medicine, “As patients with hormone-dependent cancers continue to live longer, CVD [cardiovascular disease] has emerged as a leading cause of mortality and morbidity among survivors of these cancers.”
Ironically, breast and prostate cancers are some of the most common cancers in women and men, in addition to having some of the most effective treatments. The number is of breast and prostate cancer survivors is growing. Part of the success of treatment is expressly due to the development of hormonal therapies for long-term (5-10 year) use. At the same time, the increase in CVD problems is a result of this success, because as cancer survivors age they experience greater amounts of age-related cardiovascular events than do non-cancer surivors.
So, what do you do when the treatment that’s increasing your chances of beating cancer may also be increasing your chances of a cardiovascular event? Isn’t that one of the many problems with cancer? If your treatment works well, then that opens the door to having it work “too enthusiastically”, possibly with long-lasting negative effects.
It still comes down to healthy behaviors.
The AHA statement paper cited here stresses the importance of communicating with your oncological team about CVD risk factors and possibly requesting a referral to a cardiologist, having appropriate tests conducted (ECG/EKG, echocardiogram), and–in my opinion the most important thing the survivors themselves can do–modify lifestyle (diet, exercise, smoking cessation, etc.) to maximize your chances of a cardiovascular event-free survivorship.
While it may be frustrating to think of entering into an “out of the frying pan, into the fire” scenario with a potential leapfrog from cancer to CVD, nothing is written in stone. You can make an effort to protect yourself and avoid being a statistic. Focusing on healthy living will benefit you in many ways and is guaranteed to improve your life, no matter what your risks.
~~~~~~~~~~~~~~~~~~~~~~~~~~
Link to the AHA statement: Okwuosa et al. (2021) Impact of Hormonal Therapies for Treatment of Hormone-Dependent Cancers (Breast and Prostate) on the Cardiovascular System: Effects and Modifications: A Scientific Statement From the American Heart Association. Circ Genom Precis Med, DOI: 10.1161/HCG.0000000000000082









![Chemo Fatigue: What Is It Like? [video]](https://franticshanti.com/wp-content/uploads/2022/07/howling-red-2tispdidr8i-unsplash_cropped.jpg?w=1200)